
The Signal You're Not Capturing
22% of routine mammograms contain a cardiovascular risk flag. Most health systems have no workflow to act on it.
Your health system is almost certainly running screening mammograms. If it serves women over 40 at any scale, it runs thousands of them per year.
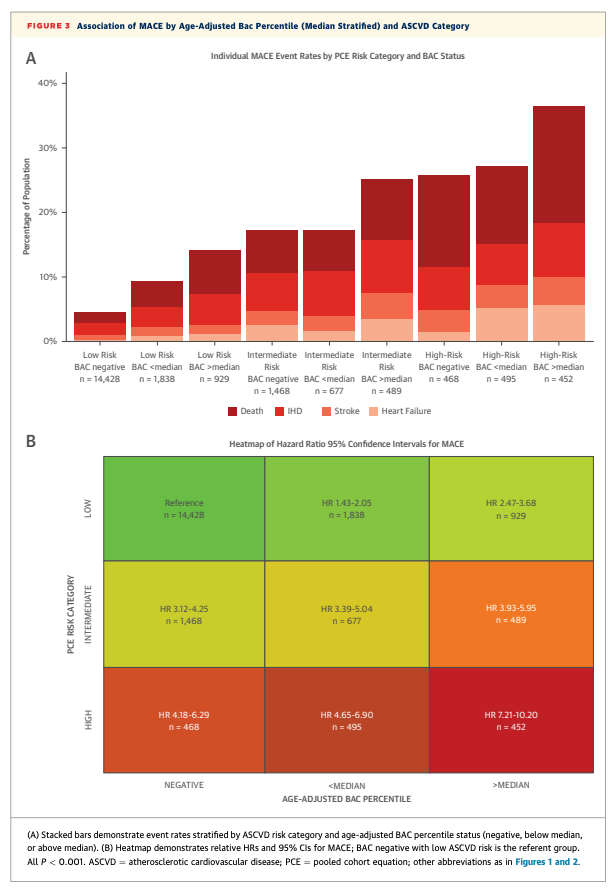
A study published in JACC: Cardiovascular Imaging adds a number worth knowing. In a multicenter retrospective cohort of 21,514 women with no known cardiovascular disease, 22.7% had breast arterial calcifications (calcium deposits in breast blood vessels, visible on routine mammograms) present, rising to 61% in older women. Nerlekar et al. found that each 10-percentile increase in an AI-scored BAC severity measure was associated with a 17% relative increase in major adverse cardiovascular events (heart attacks, strokes, cardiac death), independent of conventional risk factors. Adding BAC scoring appropriately up-classified 9% of women who subsequently experienced a cardiac event, women who had been classified as low risk by standard cardiovascular risk frameworks (ASCVD).
The imaging is already happening. The cardiovascular risk signal is on the image. It’s just not being captured.
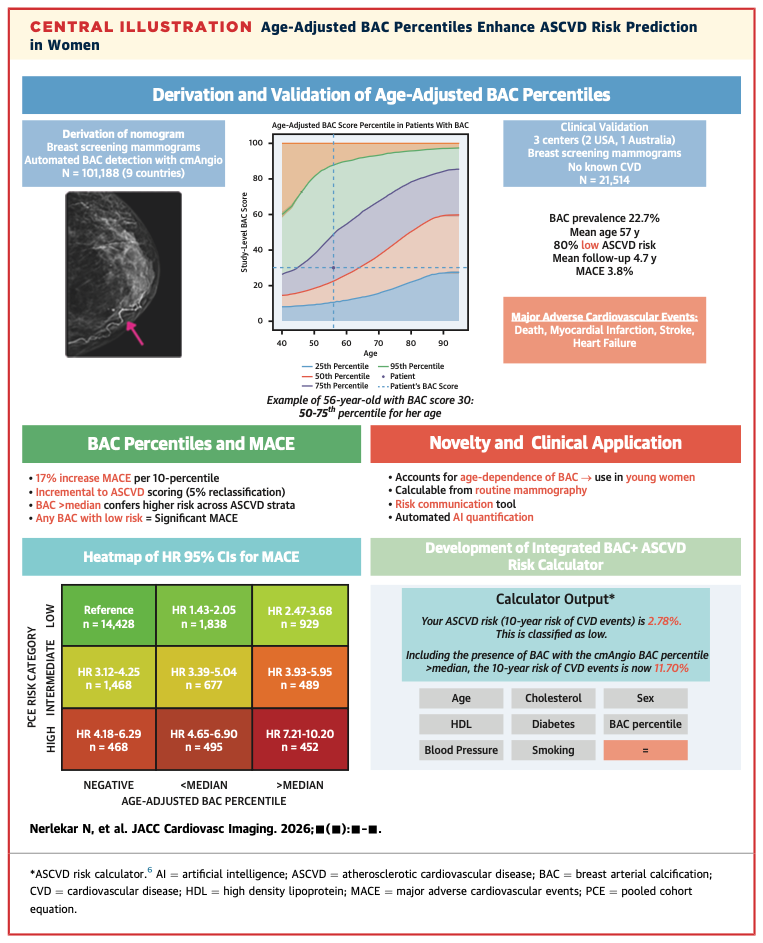
This is what capability-expanding AI looks like. The infrastructure already exists. The clinical question is new. There’s no second imaging session, no additional patient burden, no net-new capital spend. You’re running mammograms. AI reads the calcifications. A cardiovascular signal gets routed to the right care pathway.
The caveats are real. The study is retrospective, and the AI tool was built by a company affiliated with the research team. Prospective validation across diverse populations and mammography systems is the next step before this becomes a deployment argument.
But the caveats don’t change the strategic question for health system leaders: is opportunistic cardiovascular screening from routine mammography on your AI evaluation roadmap? For most systems it isn’t on the roadmap. That’s a gap worth examining. The evidence is at the stage where it belongs in an evaluation, not necessarily a contract.
For CMOs and VPs of Women’s Health: ask your radiology and cardiology leads whether BAC detection is currently on the list of AI capabilities being assessed. The reimbursement case and the care coordination model need development, but the imaging substrate question has an answer: the scan is already running.
What’s your process for getting capability-expanding AI use cases onto the evaluation roadmap?
Hit reply. I read every response.
Second Opinion is a weekly newsletter for healthcare leaders making AI decisions. Written by Jan Beger, Global Head of AI Advocacy at GE HealthCare and Executive Director of HelloAI. Views are my own and don’t represent the position of GE HealthCare or any other organization I’m affiliated with.