
The Installation Trap
US factories ran on electricity for 20 years before manufacturing productivity moved. The gap wasn't a technology problem.
In 1899, 5% of US factory mechanical drive power came from electric motors. By 1919 that figure was 53%. By 1929 it was 78%. You’d think the productivity story follows the electrification story. It doesn’t.
Average annual manufacturing TFP growth barely budged between 1899 and 1919. The twenty-year installation phase produced almost nothing. The surge came in the decade after 1919, when TFP growth hit +5.3% per year and held. The technology didn’t change. The factories did.
Steam engines had powered central drive shafts that ran belts and pulleys to every machine in the building. When factories electrified, most of them swapped the power source and kept the layout. Same floor plan, organized around mechanical constraints that no longer existed. When someone finally asked what the motors actually made possible, they scattered the motors, freed machines from the shaft, and reorganized the floor around the workflow. Manufacturing productivity followed within a decade.
I keep showing a similar chart to health system leaders. It lands every time, because they’re living in it.
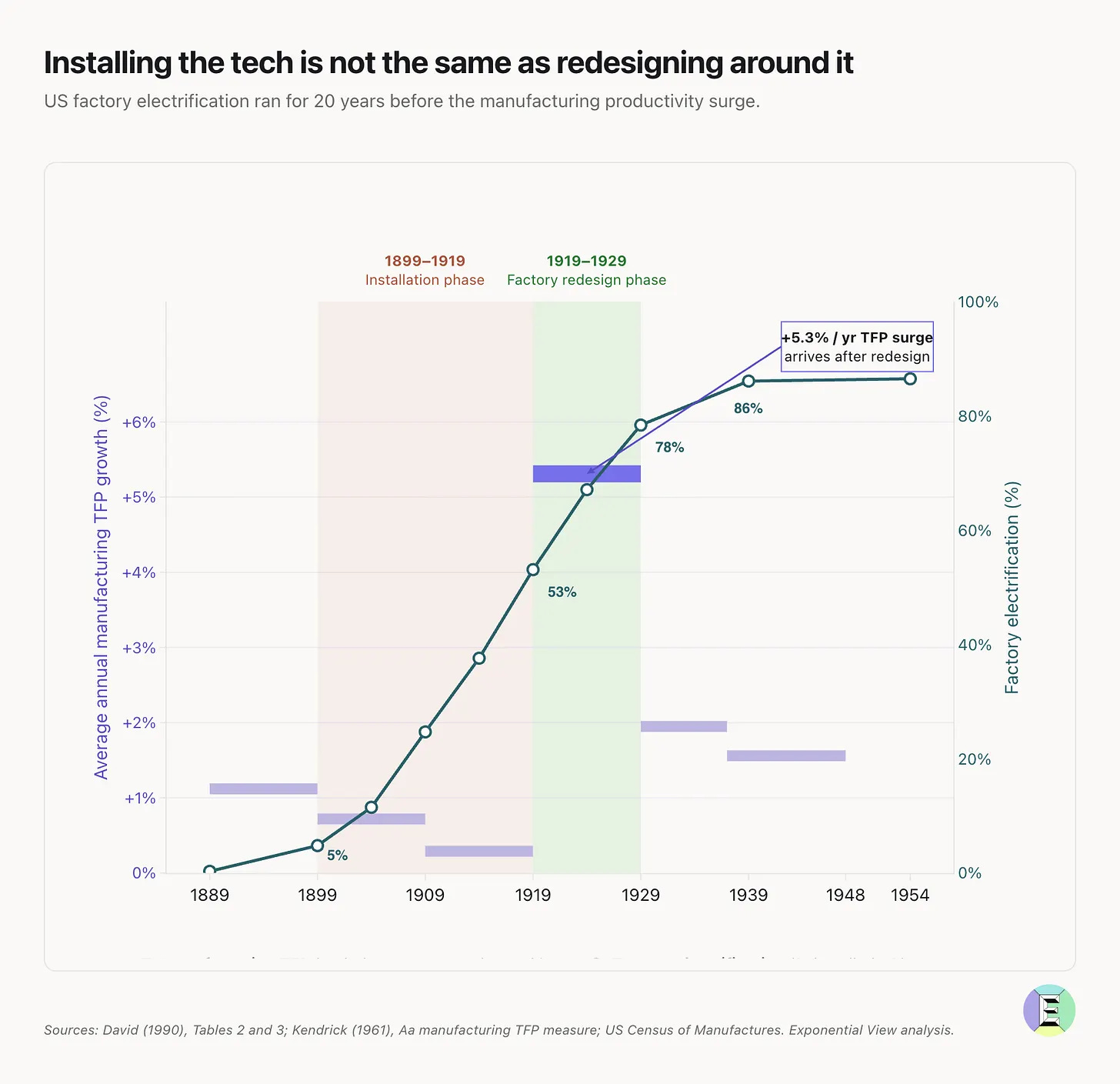
(Credit: Azeem Azhar, Exponential View, May 28, 2026.)
The chart they’re living in
Most health systems are somewhere in the 1899–1919 band right now. The technology is installed, the workflows are unchanged, and the gains are not arriving.
Stanford’s Digital Economy Lab published a study earlier this year based on 51 enterprise AI deployments across 41 organizations. Their finding: 77% of the hardest challenges in enterprise AI have nothing to do with the AI itself. Change management, data architecture, and process redesign account for the real work. One executive in the study said it plainly: “Technology wasn’t the bottleneck. Organizational adoption was the failure point.”
Catalonia registered nearly 200 AI tools in its health system by December 2025. Sisó-Almirall and Ramos-Casals, writing in The Lancet Primary Care, found exactly one fully implemented. The rest were registered. Not deployed, not in clinical use. Registered. It’s a nearly perfect picture of the installation trap: the procurement happened, the workflows didn’t change.
What redesigning actually looks like
Tom Mihaljevic, CEO of Cleveland Clinic, put it plainly on a recent podcast: “Sprinkle AI on a poorly organized health system and you get a poorly organized health system with bad software.” Cleveland Clinic spent years standardizing clinical processes and structuring data before deploying AI at scale. Most health systems have not done that work. They bought the motors and kept the floor plan.
You can see what the alternative looks like. RadNet redesigned the workflow before touching the technology. AI reads the image first. The radiologist reviews exceptions. Early deployment of See-Mode’s FDA-cleared thyroid ultrasound AI across RadNet centers demonstrated up to 30% reduction in scan time, with AI measurements accepted by radiologists without correction at a rate greater than 94%. A Nature Health study of over 579,000 women across 109 community imaging sites showed a 21.6% increase in cancer detection compared to 3D mammography alone. The algorithm was available to everyone. What RadNet changed was the operating model.
RadNet succeed for the same reason the factories succeeded in the 1920s. Someone asked what the technology made possible, then rebuilt the process around the answer.
Why it keeps not happening
The blocker is usually not who leaders expect. The Stanford study tracked resistance sources across 51 implementations. Legal, HR, Risk, and Compliance were the primary source in 35% of cases. Frontline end users: 23%.
The tools that health systems buy to reduce clinical risk get blocked by the risk function. This happens because risk and compliance teams are brought in at the end, handed something they had no part in designing, and asked to approve it. The fix isn’t to fight them. It’s to involve them earlier, give them a governance role, and tie their participation to outcomes rather than their approval to a deadline.
The other structural problem is that deployment doesn’t reduce the barriers. It adds them. Naicker and colleagues applied the NASSS implementation framework to radiology AI and found 56 barriers before deployment. After go-live: 82. Trust constrained by performance inconsistency, medicolegal uncertainty, and new accountability gaps that nobody had planned for. The factories analogy holds: putting in the motors created new coordination problems that didn’t exist with the drive shaft. Solving them required redesigning the whole floor, not just the power source. McKinsey’s research across 20 AI-leading companies (Singla et al., Rewired, 2026) found that adoption fails consistently when only the AI model changes but surrounding processes stay the same. Their example: an AI that predicts equipment failures days in advance while maintenance still follows calendar-based scheduling. The AI is right. Nothing changes. The process bottleneck absorbs everything the AI surfaces.
A practical diagnostic: pull your current AI budget and divide it. What percentage is going to software and infrastructure versus process redesign, reskilling, and change management? If the organizational side is under 50%, the investment is structured around the part that generates the least return.
The macro picture says the same thing
Torsten Slok at Apollo ran the numbers in February 2026. After three years of ChatGPT, AI remains invisible in macroeconomic data: employment, productivity, profit margins, earnings expectations outside the tech sector. Robert Solow said something similar about computers in 1987: “you can see the computer age everywhere but in the productivity statistics.” He was right, and then he wasn’t. The gains came. They just required a generation of organizations to stop doing what factories did in 1900.
The J-curve is real. It just requires the redesign to happen first.
The factories that electrified fastest in the 1880s and 1890s weren’t the ones that benefited most. They’d committed to the old layout. The ones that built from scratch, or were willing to tear out the floor, got the gains. Their advantage wasn’t access to better motors. It was willingness to redesign around what the motors made possible.
Healthcare has the same choice right now. The AI is available. The question is whether health systems install it into existing workflows or ask what those workflows should actually look like.
That’s a leadership question. Most organizations are answering the technology question because it’s easier to price.
The factories did the same thing for twenty years. Then someone moved the machines.
What’s stopping your organization from moving them? Hit reply. I read every response.
Second Opinion is a weekly newsletter for healthcare leaders making AI decisions. Written by Jan Beger, Global Head of AI Advocacy at GE HealthCare and Executive Director of HelloAI. Views are my own and don’t represent the position of GE HealthCare or any other organization I’m affiliated with.