
The Adoption Problem Is Solved
US doctors are using AI for 27 million clinical decisions a month. The question your board is asking is the wrong one.
US doctors are using AI for 27 million clinical encounters a month. The question your board is asking is the wrong one.
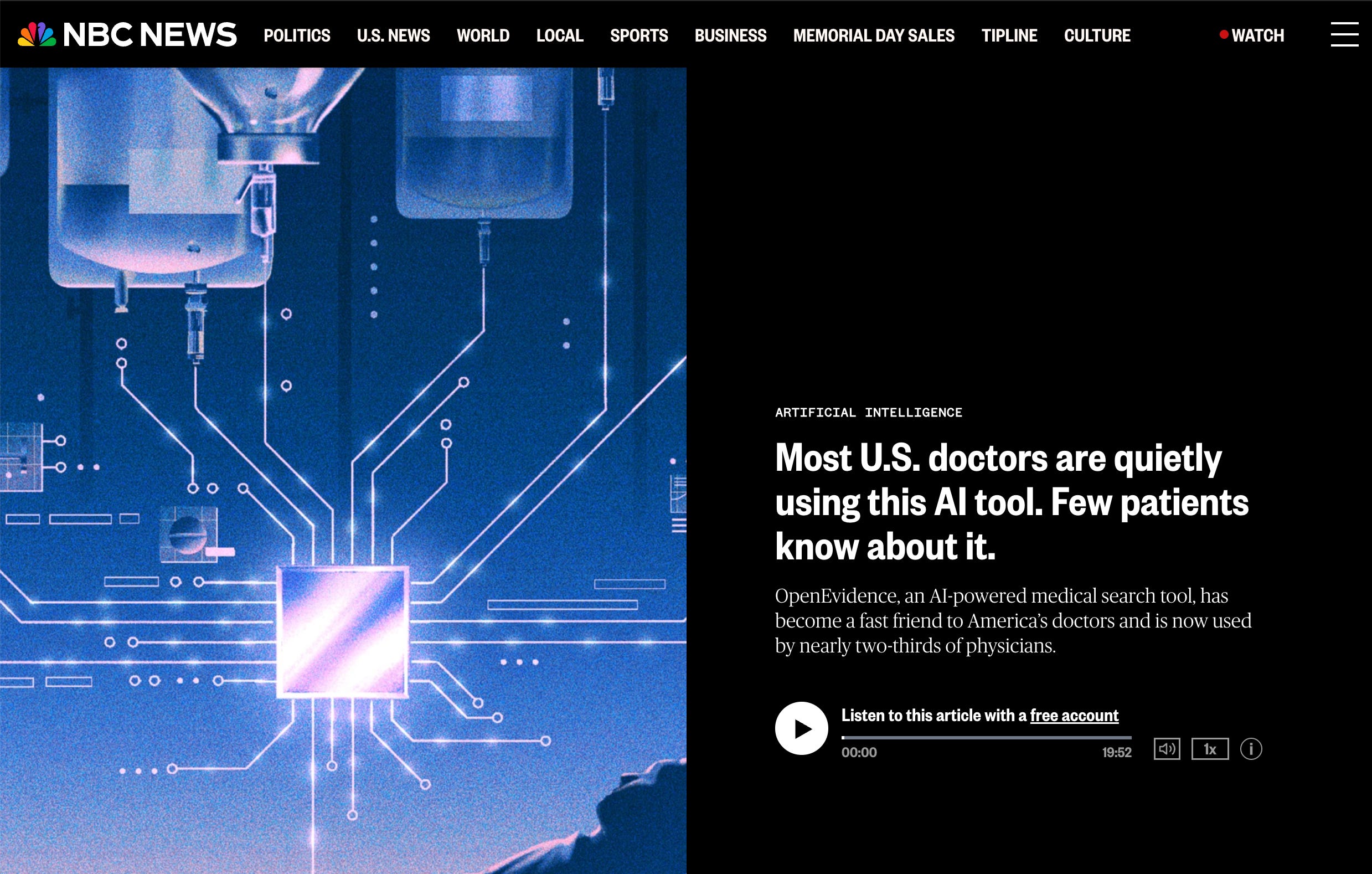
OpenEvidence reached 65% of the US physician workforce by April 2026. Roughly 650,000 physicians. 27 million clinical encounters in a single month. Drug choices. Treatment decisions. Discharge notes. The tool is free, requires only an NPI (the federal license ID every US clinician carries) to access, and not one of those physicians needed a change management program, an executive sponsor, or a procurement process to start using it.
That should reframe something for you.
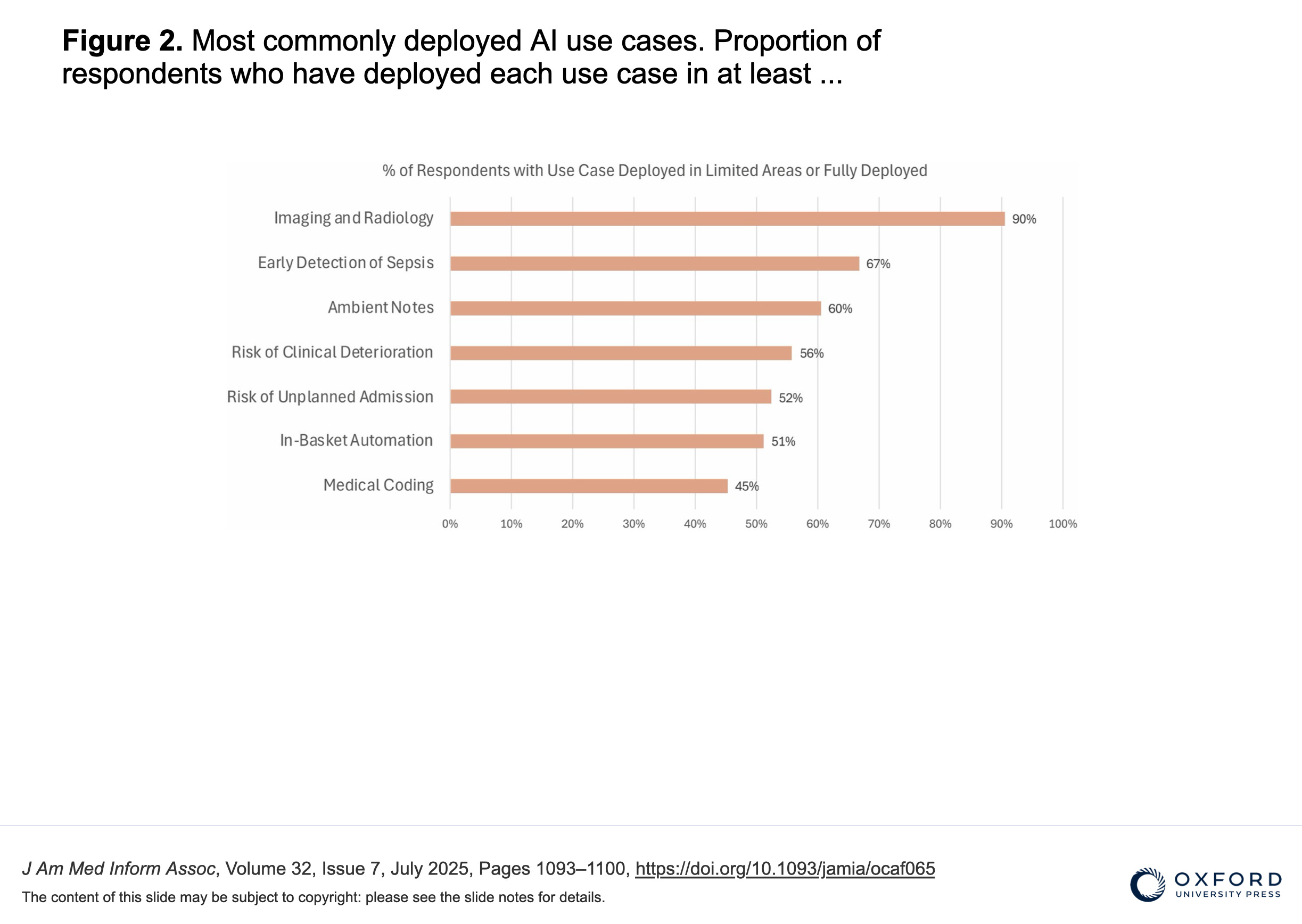
Healthcare has spent the better part of a decade treating AI adoption as the hard problem. Training programs. Pilot protocols. Clinician engagement workshops. And in the background, without any of that, 65% of the US physician workforce quietly adopted an AI clinical decision tool in under two years. That’s faster than the EHR. Faster than ambient scribes, which a JAMIA survey of 43 Scottsdale Institute health systems found had reached 100% adoption activity by late 2024, the fastest clinical technology diffusion on record.
The adoption problem is solved. Clinicians will use AI when it’s useful, free, and doesn’t add friction. They already proved it.
Which means the question your board keeps debating, “how do we get our clinicians to adopt AI?”, is the wrong question. The more pressing one: what does your organization actually do now that AI-assisted clinical decision-making is a baseline, not a differentiator?
There are three things this changes for health system leaders that most boards haven’t caught up with yet.
The liability framework was built for a different world. When a radiologist disagrees with an AI that caught something they missed, Bernstein et al. showed that simulated jurors sided with the plaintiff in nearly 4 out of 5 lung cancer cases. Not because the radiologist was negligent by any prior standard, but because AI changed what juries expect. That study involved radiology AI that went through FDA clearance and formal hospital procurement. OpenEvidence went through neither. If juries are already raising the standard for approved, vetted tools, the liability question for unapproved ones running across 27 million encounters a month is harder, not easier — and it’s one your legal team hasn’t modeled yet.
Your AI procurement strategy now has a free competitor your clinicians prefer. The tools most health systems have bought came through formal RFP processes, vendor vetting, and clinical validation exercises that took months. OpenEvidence arrived without any of that and achieved 65% market penetration anyway. That tells you something uncomfortable about how clinicians actually weigh formal procurement versus usefulness. Before your next AI vendor evaluation, ask the harder question: what would make a procured tool more useful to clinicians than the free one they’re already using?
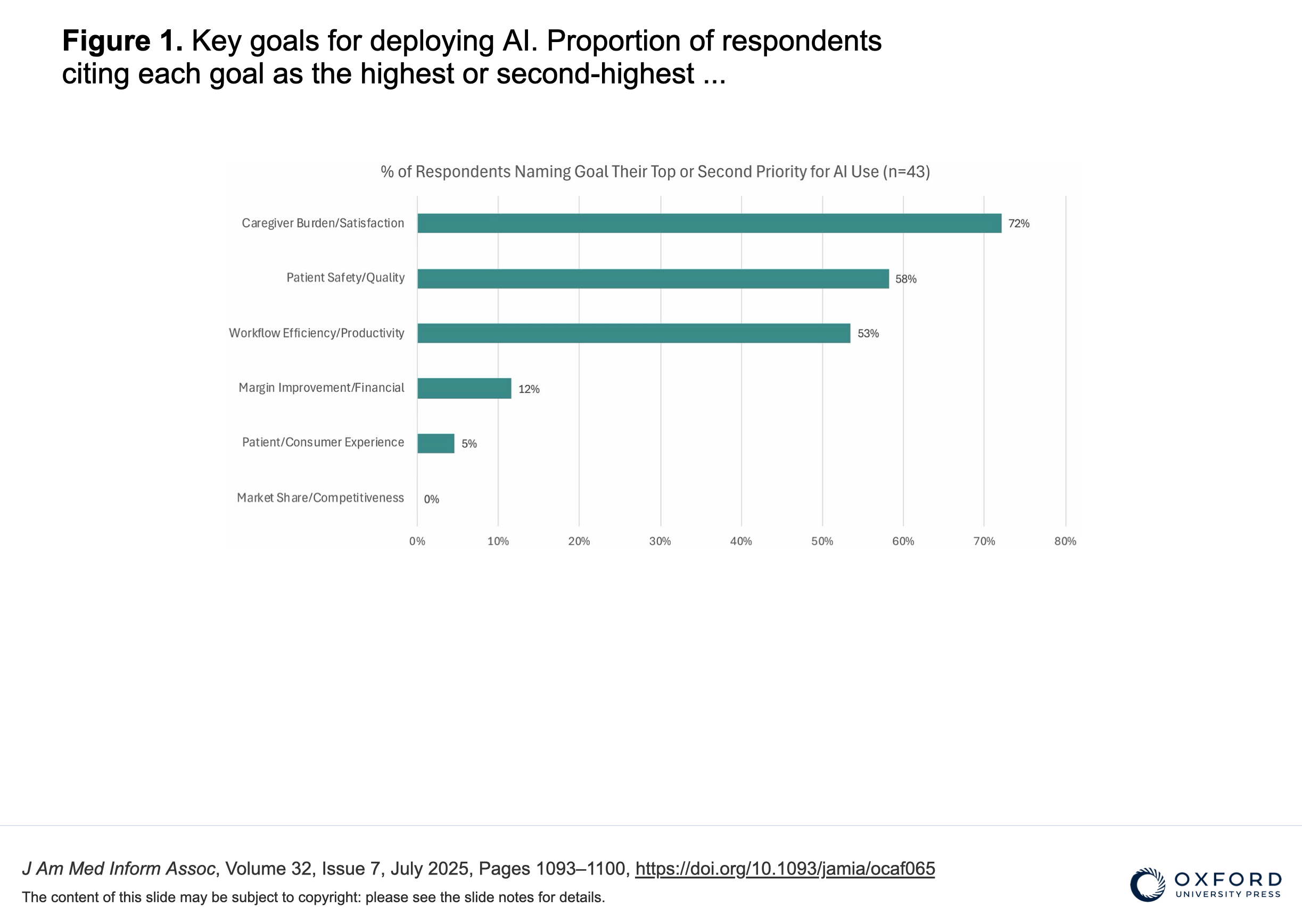
If adoption isn’t the bottleneck, where does the value actually come from? A 2026 HealthTech Magazine survey of eight healthcare IT leaders found governance named as the top concern across the board. Not because the tools don’t work, but because when AI is already embedded in clinical practice, the question shifts from “will this be adopted” to “how do we know when it’s going wrong, and who’s responsible when it does.” That’s an organizational capability question, not a technology one. The health systems pulling ahead are treating AI as enterprise infrastructure, the same way they treat the EHR: dedicated governance, continuous monitoring, a named accountability structure.
The board meeting conversation that matters in 2026 isn’t about adoption. It’s about what comes after adoption, when the technology arrived before the governance did.
What’s your organization doing with the gap between where your clinicians already are and where your governance frameworks think they are? Hit reply. I read every response.
Second Opinion is a weekly newsletter for healthcare leaders making AI decisions. Written by Jan Beger, Global Head of AI Advocacy at GE HealthCare and Executive Director of HelloAI. Views are my own and don’t represent the position of GE HealthCare or any other organization I’m affiliated with.
Adoption is no longer the question - ROI measurement and vendor accountability are. Mid-market buyers need frameworks for evaluating AI outcomes, not just AI features.